1. 正常的average normal corneal thickness: 540μm
2. AGIS結論:眼壓固定小於18,平均12.2,有較小的fluctuations者會有better outcome。
3. CNTG的target IOP reduction是30%
4. GLT(Glaucoma Laser Trial)結論:laser與medical therapy的治療組結果相當。
5. exfoliation syndrome患者的AC angle會比較shallow,另外會有spontaneous lens dislocation, earlier cataract formation, 白內障手時Vtreous loss機率較高, IOP變化較大。
6. pigmentary dispersion syndrome好發於myopes,使得early detection較為困難。laser iridotomy不能增加AC depth, 其AC angle顏色會變深,laser能量可以減低。
7. aqueous humor每分鐘有1%的turnover
8. angle-closure病人的axial length較短, AC depth較淺, lens ant. curvature增加, cornea diameter較小,radius of curvature也小(curvature較大)。
11. Sturege-Weber無遺傳型式(sporadic),unilateral, 男女一樣多, 會造成open-angle glaucoma (EVP增加), 是infantile glaucoma的重要成因之一。
13. foreshortening of the conjunctival fornices不會增加episcleral venous pressure.
14. automated perimetry使用了"staircase" strategies來評估不同視位置的threshold sensitivity。
16. 隨著年紀增加 AC angle pigmentation也會增加
17. Fuchs endothelial dystrophy若造成glaucoma,屬於angle-closure,而非open-angle
18. anterior optic nerve (intraocular portion)的diameter是1.5mm左右
20. adult-onset glaucoma遺傳型為AD
21. 已知與congenital glaucoma相關的三種genes,合計佔了congenital glaucoma總量的75%。
22. DM不是glaucoma明確的risk factor
23. aniridia與PAX6相關
24. GLC1A gene與Juvenile/Adult open-angle Glaucoma有關,與TIGR/myocillin protein異常有關,位置在1q23。超過40種mutations(而非single, specific mutations)
* 目前已知之Glaucoma Gene
GLC3A,3B for congenital glaucoma是AR,其它都是AD
GLC1A, 1q23 for Juvenile Glaucoma
NNOS for PACG
4q25 – Rieger syndrome
25. 女人的AC比男人還要shallow
26. trabeculoplasty經過10年的longterm追蹤,成功率只有30%
27. 對單一青光眼藥物不良反應不是incisional surgery的理由(因為可以換藥)
28. trabculectomy加上mitomycin-C會使得bleb less hyperemic
29. elevated IOP despite maximal medical therapy應先考慮trabeculectomy,而非直接做tube shunt surgery
32. low scleral rigidity者易在Gldmann applanation tonemetry時低估眼壓。
33. occipital infarction可能產生homonymous hemianopia
34. glaucoma的histologic changes不包括loss of outer nuclear layer of the retina
35. NVG不會造成pupillary blcok
37. Laser PI也可能造成malignant glaucoma
38. homocystinuria通常與lens subluxation有關,而與trabeculodysgenesis無關。
39.betaxolol是selective beta1 agonist
40. pilocarpine是diret cholinergic agonist(所以不會間接地inhibit cholinesterase)
41. ICE的PAS會跨過Schwalbe's line
42. Fuchs heterochromic iridocyclitis不會形成PAS,與angle-closure亦無關( Fuchs endothelial dystrophy則與angle-closure有關)。
43. phacolytic glaucoma沒有KP,而phacoanaphylaxis會有KP。

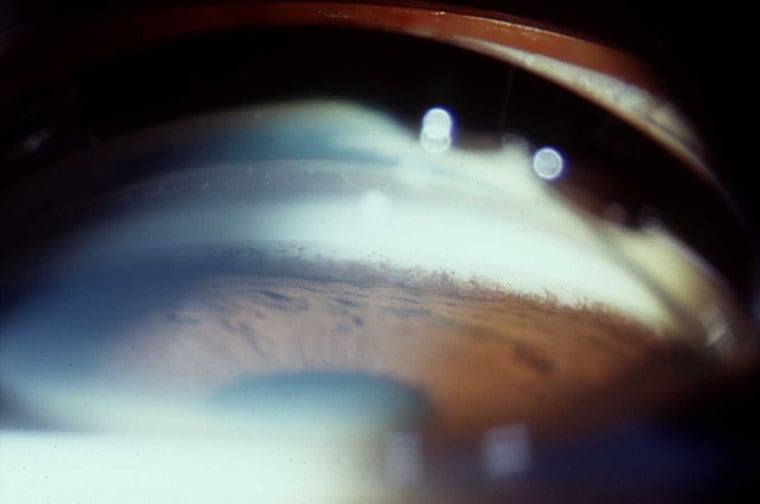 Angle Recession
Angle Recession